If you're a health professional you should know that you can't implicitly trust medical news outlets. They may be manipulating you!
Cholesterol as a Nutrient: Evidence Against the Lipid Theory of Heart Disease
Table of Contents
- Does cholesterol cause heart disease?
- When Cholesterol Takes Center Stage In Heart Disease
- Question 1) What is cholesterol?
- Questions 2&3: What kind of cholesterol is good, what kind is bad
- Questions 4 & 5: What is a high cholesterol number and how can you lower it naturally?
- Question 6: What is oxidized LDL?
- Question 7) What causes heart attacks and strokes?
Does cholesterol cause heart disease?
For decades, Americans have been taught that cholesterol is a primary cause of heart attacks and strokes, and that lowering cholesterol is essential for cardiovascular health. This belief is so deeply embedded in medical training and public health messaging that it is rarely questioned. Yet when the evidence behind these assumptions is examined closely, the story becomes far less straightforward than most people realize.
This article is the first in a series that explores how cholesterol came to be viewed as harmful, why that belief persisted, and what the scientific record actually shows. It traces the origins of the lipid theory of heart disease, the role played by influential institutions, and the consequences—intended and unintended—of basing national nutrition guidance on this framework. Along the way, I will explain how I came to re-evaluate cholesterol’s role in human biology and why I now view it as a misunderstood and essential molecule rather than a dietary villain.
We will begin by addressing the basic questions that shape nearly all conversations about cholesterol and heart disease.
This article is continued below...(scroll down)


It helped. I feel great.
"It’s helped. I feel great."
Kobe Bryant
NBA baskeball player

This has been life changing
"Let me tell you this has been life-changing. I have all of her books, in audible and ebooks! I have gotten rid of all the hateful 8 oils. I have trained my body to eat its own previously toxic body fat. Download that pod it's a game changer!"
Megyn Kelly
Broadcaster / The Megyn Kelly Show

Life changing
Deep Nutrition changed my life.
Jesse Watters
Fox News Primetime host
Saved my life
I would like to thank you for literally saving my life. Back in February, I had to be hospitalized while on vacation in Phoenix with an A1C of 11% and had to start taking 2 types of insulin and 2 other meds. I read the Fatburn Fix in April, and followed the program to a tee, and I’m down by 15 pounds, 6.8 A1C, and only one once weekly diabetes medicine. Prior to reading the book, it was almost impossible for me to lose weight as a diabetic.
Leontyne Tompkins
I feel free
For the last month, I have really been reading all labels on everything. I have completely remove those 8 oils you talk about. I must tell you, I feel great! I have more energy and I am now 197 lbs (have always been around 205 to 210lbs). I eat potatoes with real butter, grass fed steak, pasta with the right toppings. I eat everything! I seem to crave less sugar. I love it!
Robert Kirkendall
I feel so much better
I had terrible aches and pains everywhere in my body, my hands, shoulders and knees. I feel so much better and the way I feel is motivating me every day! Thank you
Mike Deb Wootan Burcin
Better than ever
I am an anesthesiologist in Orlando and a huge fan of both of your books! I have been incorporating your principles for the last 10 months and feel that my health is better than ever.
Marnie Robinson, MD
My allergies disappeared
The biggest difference for me (and a surprising one) is that my allergies have almost completely disappeared! This is a big deal for me, because I’ve had allergies most of my life and they have often affected what I do which is a teaching music in [a public school district]. In general, I feel much better and have more consistent energy throughout the day.
Erica Turrell
Heart Palpitations have Stopped
I’ve lost 20+ pounds (also fasting 16-24 hours daily) and haven’t had palpitations except for one occasion — I had a mini bag of Fritos for the first time in July. And, I feel better now on a daily basis than I ever did all through college.
Mike Wright
Deep Nutrition and Fatburn Fix reader

I’ve lost over 50 pounds
I’ve lost over 50 pounds. I’m 56 years old. Cutting processed food and unhealthy fats from my diet was one of the first things I did on my health recovery journey...I went cold turkey off the bad oils. Emptied my pantry into the trash and just started eating real food
Mitzi Wilkinson Champion
Knowledge I didn’t know I needed
Your Fatburn Fix book is amazing, my friend. Thank you! I’m an Functional Nutritional Therapy Practitioner and I know my stuff. This is the extra layer of knowledge I didn’t know I needed. Well done!
Jennifer Dillman
Fatburn Fix reader
Lost a solid 20 lbs and my bloodwork is great
I have lost a solid 20 lbs and my bloodwork (after 3 months of eating your way) was even better! I was metabolically healthy (per your book) before I read your book, but barely. Lowering my weight, sealed the deal! I have been talking about you and your book to anyone who will listen...Thank you for all you’ve done and what you continue to do! You are changing lives for the better!
Missy Cramer
FatBurn Fix reader
Lost 20 lbs I could never shed
I love your Fatburn Fix! Has helped me so so much! I have had the dreaded weight all my life - 20 or so pounds I could never shed. I have lost that now. I only eat 2 meals a day lunch and dinner with a glass of milk or cappuccino around 4 to hold me over. No snacking and not bad oils. It has been the key to unlocking my fatburn. I work out in the am and believe I am burning fat for energy not from food!
Lauren Smith
I feel great
My waist is four inches smaller. I feel great and many of the minor aches and pains that I had (knees and lower back) are gone. Also, my muscle tone is amazing, even though I have not increased my workout routine.
Richard Janelle
Completed Dr Cate's online course

The go-to for strength and conditioning coaches
Whenever I advise my clients about eating to perform I go straight to what I have learned from Dr. Cate. Her book Deep Nutrition has become the go-to for strength and conditioning coaches across the country.
Kent Matthes
Major League Baseball Agent with WME Sports

Dismantles the lie
Dr. Cate dismantles the lie that seed oils are healthy, which may the biggest lie about nutrition and health because it’s so insidious.
Ken D Berry, MD
Author of Lies My Doctor Told Me

She knows the chemistry
Dr. Cate alerts us to the harms of seed oils and she’s convincing because she knows the chemistry better than anyone.
Dr. Drew Pinskey, MD
Globally recognized internal medicine and addiction medicine specialist, media personality, LoveLine Host, and New York Times bestselling author

No one is better at communicating nutritional truth
Dr. Cate has had the single greatest impact on how we talk to people about fueling for both performance or durability. While we all are a little unique, the foundational principles of human nutrition are immutable. If you are looking to create a more durable, resilient body, no one is better at communicating nutritional truth than Dr. Cate.
Dr. Kelly Starrett
Physiotherapist coach and New York Times and Wall Street Journal bestselling author

Highly recommend The Fatburn Fix
Dr. Shanahan has had a significant impact on my practice of medicine. I am known as a Low Carb Doctor, but I never really appreciated the negative effects of processed seed oils on the health of my patients. I highly recommend The Fatburn Fix to my patients and have a loaner copy in my waiting room. It is amazing how quickly blood sugars and overall health improves with cutting seed oils. It is not just about the carbs!
Dr. Brian Lenkzes, MD
CEO of LowCarbMD San Diego, co-host of Low Carb MD Podcast and host of Life's Best Medicine Podcast

Respected in the sports world
Dr. Cate reordered my diet when I was with the L.A. Lakers, and the benefits, for me personally, were felt immediately and have served me to this day. I’ve come to take real food so seriously I started a small family farm. I know of no M.D./nutritionist more respected in the sports world than Dr. Cate Shanahan.
Chris Kaman
NBA Player

Brought seed oil issue front and center
Cate brought the seed oil issue front and center. Healthy fats matter. So much so that I created an entire product line to swap out bad fats with good.
Mark Sisson
Founding Father of the Primal/Paleo Movement

Optimal health starts with food
If you want to understand how optimal health starts with food, start with Dr. Cate. Her book Deep Nutrition leaves you with an appreciation of the profound relationship between our genes and the planet, inspiring us to be good shepherds of both.
Dallas Hartwig
Attribution author of The Whole 30

Helped me with endurance
Deep Nutrition really helped me with endurance. I started to feel better as a player. I was able to run more, I was able to be more active …and I just decided to keep going with it to this day.
Dwight Howard
NBA Player

Silver bullet for me
Dr Cate’s teachings helped me lose 60 pounds like it was nothing. It was like a silver bullet for me.
Paul Grewal, MD
Dr Grewal Internal Medicine, MD, author of Genius Foods
Radically improve your health…
Dr. Shanahan has provided a solid reference that deserves a place in the library of anyone who is seriously interested in nutrition. Her perspective on the vital role that healthy fat has in our diet is novel and, if implemented, can radically improve your health.
Dr. Joseph Mercola
Author of Fat for Fuel and Founder of Mercola.com

Pull up a chair…
I have based my work on the idea that getting the right kinds of healthy fats into your body and avoiding the worst fats is essential to optimal health. I've interviewed dozens of the world's top experts about this, and I know of no one who speaks more eloquently on this topic than Dr Cate. If she’s talking fats, pull up a chair. Take notes.
Dave Asprey
Author of the Bulletproof Diet
The key to unlocking my fatburn
I love your Fatburn Fix! Has helped me so so much! I have had the dreaded weight all my life - 20 or so pounds I could never shed. I have lost that now. I only eat 2 meals a day lunch and dinner with a glass of milk or cappuccino around 4 to hold me over. No snacking and not bad oils. It has been the key to unlocking my fatburn.
Lauren Smith
Saved my life
I would like to thank you for literally saving my life. Back in February, I had to be hospitalized while on vacation in Phoenix with an A1C of 11% and had to start taking 2 types of insulin and 2 other meds. I read the Fatburn Fix in April, and followed the program to a tee, and I’m down by 15 pounds, 6.8 A1C, and only one once weekly diabetes medicine.
Leontyne Tompkins
> Tears of joy
I'm crying tears of joy and appreciation for all you've done for me and my health! Without Deep Nutrition and Fatburn Fix, I would literally still be in the vicious cycle I'd been fighting all my life! In a nutshell - I am no longer a compulsive overeating addict suffering under the crushing 'thumb' of all food and alcohol.
Penni Wicks
- What is cholesterol?
- Which is the good cholesterol?
- Is LDL cholesterol good or bad?
- What is a high cholesterol number?
- How to lower cholesterol naturally?
- What is oxidized LDL?
- What causes heart attacks and strokes?
We all hear that having a high cholesterol level is dangerous, don’t we?
Unless you’ve been living under a rock, you’ve heard a thousand times that higher than “normal” cholesterol levels cause heart attacks and strokes. We need some cholesterol, but most of us get too much–so we hear.
We don’t often hear where this idea that having a high cholesterol level is bad comes from. Or who it came from. And most importantly, what were that person’s motivations and possible biases?
At a crisis point in my career, I began to doubt the idea that high cholesterol levels were bad and realized I needed to know the answers to these and other basic questions before I could feel confident dishing out any more dietary advice. Before I could feel comfortable abandoning what I’d been taught, I had to answer many technical questions on my own, since the medical leaders in this area had proven themselves unreliable. Thankfully, I had the relevant chemistry training to understand the many thousands of articles that helped me find the answers I needed. This information changed everything about how I practiced medicine, and it has since changed many thousands of people’s lives for the better.
For help understanding the flawed nutritional principles disseminated by Harvard and the AHA may have affected your health, and how to recover the fastest, please schedule a consultation.
Today’s article is my attempt to summarize the most important points about cholesterol that very few doctors have taken the time to understand. The next two articles after this one will cover important moments in medical history that few doctors are aware of, and that serve to turn well-intentioned doctors into servants of the sickness industry. If this story of the AHA’s absolute power to control what doctors think—especially when it comes to cholesterol— makes sense to you, my hope is that it will arm you with the confidence you need to prevent well-meaning but poorly informed medical doctors from giving you diet or drug prescriptions that will jeopardize your health.
When Cholesterol Takes Center Stage In Heart Disease
As recently as the 1940s, only a few people on the planet even knew what cholesterol was. Doctors went about their days enjoying foods loaded with cholesterol and fats that raise blood cholesterol levels, just as all of humanity has since the beginning.
The seeds of change were first sewn in 1948, during a meeting of the American Heart Association, when members assembled and decided to reinvent the organization. Instead of raising money from member physicians, the leadership wanted to start forging corporate partnerships. A short while later, the AHA had attracted a wealthy benefactor who, as it happened, wanted to boost sales of liquid vegetable oil for cooking and salads, and margarines made with hydrogenated (solidified) vegetable oil.
Fast-forward 70 years.
Today, I doubt you can find an adult in this country who hasn’t heard of cholesterol. Most people I speak with about their cholesterol blood tests are understandably worried about their results—and little wonder. The information we get from the media, food labels, and blood test reports has programmed not just doctors, but everyone to be afraid of cholesterol. This fear influences our daily food choices and our shopping and snacking habits. It’s a big part of everyone’s life.
We’re so scared of cholesterol, we don’t even ask Google the normal questions, like “what is cholesterol” or “is cholesterol bad.” We jump right to search phrases like “how to lower cholesterol levels” and “new cholesterol drug,” according to google trends. When you click on “how to lower your cholesterol,” the typical article will tell you to start cutting out saturated fat and replacing it with polyunsaturated fats.
That’s a strategy I myself used to believe in. But some twenty years ago I learned it was all based on a house of cards because the very notion that we need to lower cholesterol is not grounded in solid science.
The word “myth” gets tossed around often regarding the cholesterol theory of heart disease, but myth refers best to either something completely mystical which has no known basis in accepted fact or a conclusion based on lack of experience or knowledge. What we’re all taught about cholesterol, starting in grade school and continuing all the way up through graduate medical training, is better described as a fallacy, because these teachings are based on unsound, flawed, and illogical arguments. You could also just call it a big fat lie.
I didn’t set out to become a rebellious doctor, but once I learned the truth about cholesterol, I had to decide if I was willing to risk my career to do the right thing for my patients. I quickly discovered that the cholesterol lie was about much more than cholesterol, as you’ll see. I ultimately decided that, in spite of the risks, to continue to practice according to conventional wisdom was no longer defensible. I’ve since extracted myself from the systems that reward doctors for dispensing diet advice that sets your health trajectory on a downward spiral. Now, I’ve made it my mission to free as many people as I can from this medical lie to give you back what you’ve been missing. So I hope this article will help you.
To begin with, let’s discuss cholesterol itself.
Question 1) What is cholesterol?
Cholesterol is a chemical we can’t live without. It’s a big flat molecule shaped like a segment of honeycomb that solves a lot of problems for your body’s cells. Cholesterol is so basic to life on Earth that it’s been with us for 2 billion years, when Nature upgraded cells from single chamber to multi-chamber, inventing what we call “true cells” (eukaryotes) and is now one of the basic ingredients making all plant and animal life (yes plants make cholesterol) possible. It strengthens your cell walls (called membranes), helps the doors of your cells open and close, can be turned into hormones (including vitamin D, cortisol, estrogen, and testosterone), can talk to your DNA, and is required to help break down your food. Lacking cholesterol impairs growth, digestion, reproduction, injury repair, adaptation to stress, and fighting off infections. Plus it waterproofs your skin keeping your bodily fluids inside, where they belong, and keeps you from dehydrating you into a human prune. Keeping your brain healthy also requires massive amounts of cholesterol, and limiting your brain’s ability to make cholesterol will visibly shrink it. (Most doctors will attribute a reduction in someone’s brain size to age-related dementia.)
For the purposes of this discussion, the most important thing to know about cholesterol is that it helps stabilize the vehicles that carry fat through the bloodstream, ensuring these nutrients arrive at their destination. The vehicles that carry cholesterol and fat through the bloodstream are called lipoproteins. They come in many shapes and sizes depending on whether they were made in your intestines, your liver, or elsewhere.
Lipoproteins are Delivery Vehicles for Cholesterol and Fats
Lipoproteins are made of lipid and protein. The lipid fat is stabilized by cholesterol. The proteins are on the surface and help to make sure the lipid fats and cholesterol get to the parts of your body that are in need of fats and/or cholesterol. (See image below, of LDL particle on a bike sporting an Uber Eats hat)
Lipoproteins distribute the fat and cholesterol you eat throughout your body. They also distribute fat and cholesterol your body makes in the liver or other organs. They’re essential to the process of nourishment.
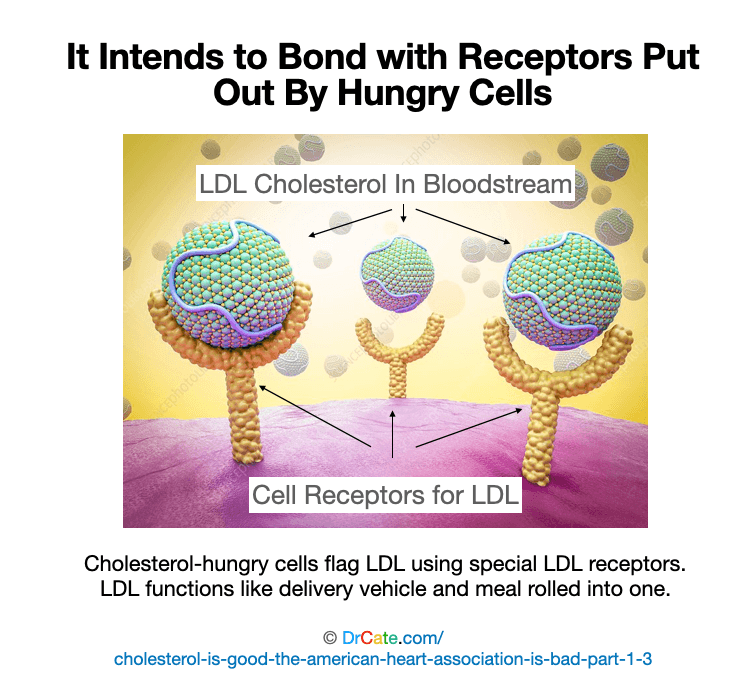
Without the biggest lipoproteins, called chylomicrons that carry the fat coming from your last meal, the fat that you eat would build up around your intestines and kill you. Without the medium size lipoproteins, called VLDL (very low-density lipoprotein), that carry fat out of the liver, the fat your body releases during exercise would build up in your liver and kill you. Without one of the smaller lipoproteins, called LDL (low-density lipoprotein) that transfers cholesterol (and a little bit of fat) out of your capillaries, the many tissues of your body that need cholesterol would never get enough, which would restrict growth by restricting cell division and repair, and ultimately kill you.
You’re getting the picture, yes? No cholesterol, no you.
But wait, you might be thinking, sure cholesterol can be good, still, can’t there be too much of a good thing?
That’s exactly the argument the American Heart Association wants you to buy into. What the AHA doesn’t want you to consider is that Nature isn’t stupid. Your body regulates the production of pretty much every important molecule, ramping up production when you need more, and putting on the brakes when you need less. And that means if you’ve been following the kind of diet I recommend for a while (how long it takes depends on your body burden of PUFA, discussed in the FATBURN Fix) and if you’re not a smoker, then your bloodstream will never contain more cholesterol than it can safely handle. Period. Even if your cholesterol numbers register in the danger zone according to standard labs—more on that below.
The next two questions are best answered as a pair:
Questions 2&3: What kind of cholesterol is good, what kind is bad
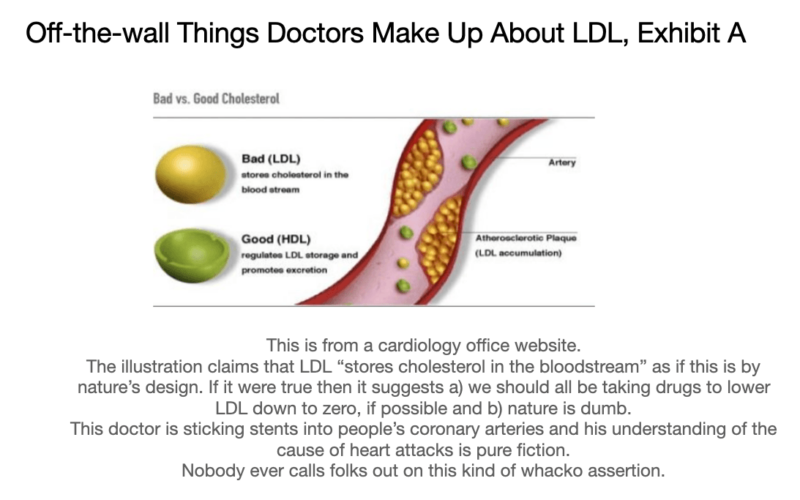
Most doctors are taught LDL is “bad” and HDL is “good.” This sounded reasonable enough to me, back when I first heard about it. To be honest, I never thought much about it. I simply repeated it, over and over. Some doctors who think about it a little more try to invent their own reasons for calling LDL bad cholesterol, like the one in the illustration below. Most such made-up ideas are silly and, by the time you finish this article, you’ll know more about cholesterol and the real cause of heart attacks than most doctors.
The real answer is that neither LDL nor HDL cholesterol is always good or bad. It depends on the particle’s composition, which depends on what you’ve been eating. If your diet has been good, both these particles are good. If your diet has been not-so-good, then both LDL and HDL are not-so-good, and both can end up damaging your arteries, with deadly consequences.
The AHA does not want you thinking about it this way. They don’t want you thinking holistically. Actually, as far as I can tell they don’t want you thinking at all. They’d rather you take their advice without question, just like I did in the early years of my medical career. They’ve got most people so scared of cholesterol they are too panicked to think and if the google search frequency is any indication then the AHA has made people more afraid of cholesterol than of the heart attacks it supposedly causes.

Whether your diet is good or not-so-good depends not on how much fat or cholesterol you eat, but on what kinds of fats you eat. Certain fats are prone to reacting with oxygen and when these reactions take place inside your lipoproteins, they make your lipoproteins toxic. The more of these reaction-prone fats you eat, the more toxic lipoproteins you have circulating in your arteries, and the more problems your arteries will have. (More on this process, called oxidation, below)
If your diet is loaded with the wrong kinds of fats, then no matter your HDL or LDL numbers, your arteries are in trouble. On the other hand, if you eat the kind of diet I recommend, including good fats (from this list) and avoid the bad fats (from the same list), and eat foods rich in the other nutrients required to be healthy, then you don’t have to worry about these little fires starting in your arteries, no matter how much cholesterol there is.
In other words, the HDL and LDL numbers don’t tell you what you need to know. What you’ve been eating makes all the difference. (There are other numbers you can track to understand your current metabolic health in more depth, and we’ll touch on those later on.)
Another important factor is how fast your body can put out the oxygen reactions once they start. If you’re a smoker, your body is always fighting these little fires, and it’s hard for the firefighters (your antioxidant enzyme systems) to keep up. If your diet is low in vitamins, minerals, and certain kinds of protein, your body can’t manufacture enough of the fire-fighting enzyme systems. This is a big reason why smoking and malnutrition are both important factors leading to heart attacks and strokes.
The next two questions are also best answered as a pair.
Questions 4 & 5: What is a high cholesterol number and how can you lower it naturally?
The politically correct answer to this question has crept lower and lower over time. When I first entered medical school, any cholesterol number under 300 wouldn’t have raised the doctor’s eyebrows. Over the past few decades, the goalposts have shifted. Today, if your total is over 200 or your “bad” cholesterol is over 100 the lab will give it a red flag and your doctor will probably start warning you off steak and lobster. But none of those red-flag numbers were grounded in solid science.
The real answers are 4) total and LDL cholesterol don’t correlate well with risk. If anything, higher numbers seem to reduce mortality. Watch a cardiologist talking about that here. And 5) You don’t want lower cholesterol. So don’t lower it. Period.
Still, there is a lot to be learned from each of the numbers reported on a cholesterol test, as long as you know how to interpret them. These numbers can all tell you something important about the state of your metabolism. I teach folks how to interpret their numbers when I work privately with patients, and will be offering a group class starting in January 2021 (please subscribe to learn more if you are interested).
My most recent total cholesterol was 263, LDL cholesterol was 177, HDL was 83 and triglycerides were 65. Even though my own personal physician wasn’t happy, these numbers indicate overall good metabolic health.
I’ve met folks whose low numbers gave them a false sense of security that their diet was healthy, and unfortunately suffered a heart attack or a stroke. This happens quite a lot. To keep doctors from thinking about all these people with perfect numbers who nevertheless tragically suffer and sometimes die, the AHA explains that this happens due to something they call “residual risk.” It’s a term I think they came up to try to convince us that the AHA has a handle on the situation and that we should probably all stay tuned to their channels because pretty soon now they’ll be coming up with a solution. In other words, it’s another way of preventing doctors from thinking for themselves.
Residual Risk Means No Matter How Low Your LDL, It’s Never Low Enough
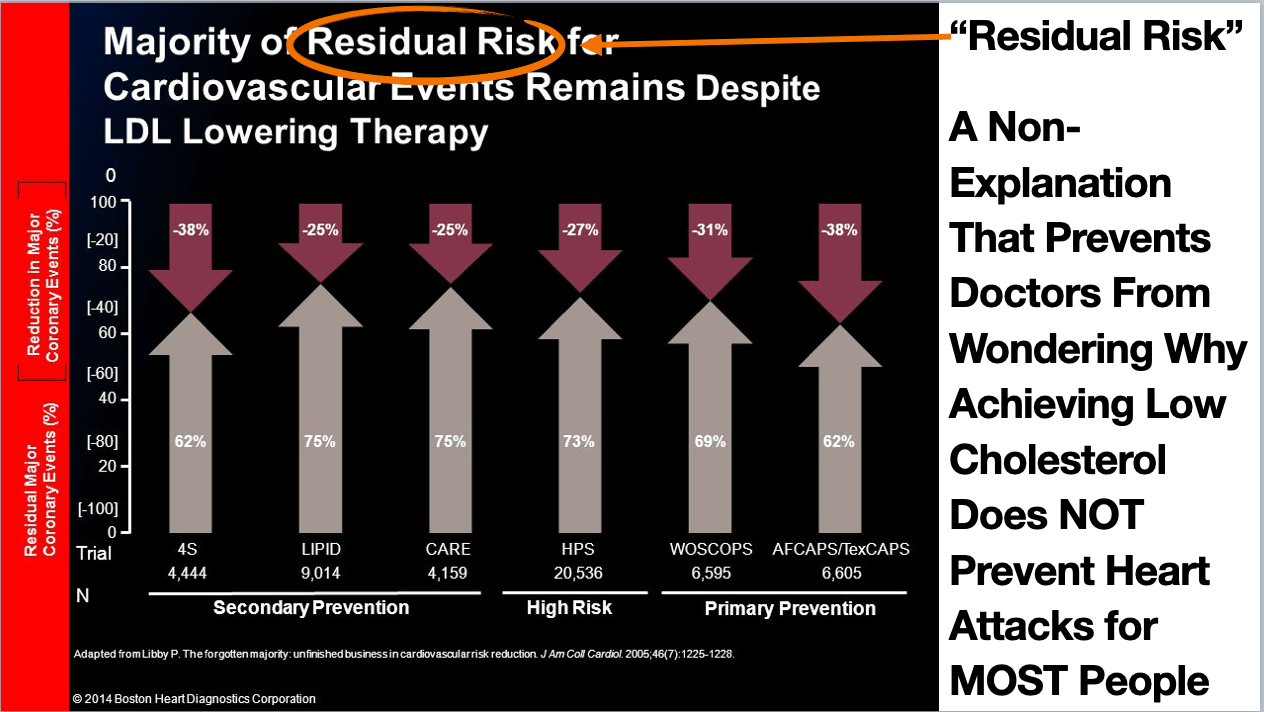
Having heart attacks in spite of very low LDL is a common occurrence. Around 2010, a majority—roughly two-thirds—of people who’d had a heart attack had achieved low cholesterol numbers that were considered ideal at the time. So rather than questioning the idea that LDL cholesterol is the cause of heart attacks, the AHA and other medical leadership upped the ante, moving from specific numerical goals to simply focusing on maximizing the dosage of cholesterol-lowering drugs.
Given how often low cholesterol failed to prevent heart attacks from happening, you’d think more doctors would have started questioning the benefits of lowering cholesterol. But the AHA nipped that in the bud, inventing a pseudo-sciencey explanation they call “residual risk.” “Residual risk” means that there are factors other than the absolute LDL number that need to be taken into account, like smoking, HDL level, triglyceride level, and inflammation. Taking these other factors into account is a good idea. But what’s even better is gaining a better understanding of a chemical process called oxidation.
Athletic trainers often warn their clients “You can’t out-train a bad diet.” This line of thinking offers a much better explanation for the cause of residual risk: You can’t out medicate a bad diet.
This begs the question, though, doesn’t it: What makes a bad diet ‘bad’? It all boils down to oxidation.
Question 6: What is oxidized LDL?
Oxidized sounds like oxygen, doesn’t it? That’s not for “nuthin,” as they say in Jersey. Oxygen in the air reacts with wood and burns or oxidizes it. Getting to know oxygen a little better is going to get us to the true cause of heart attacks and stroke.

Oxygen is like a bully molecule. It has a tendency to attack weaker molecules. Oxygen is at once crucially important to most living creatures, yet also so dangerous that it almost destroyed all living things on planet Earth about 2 billion years ago. The only thing that enabled our distant ancestors to get past this dangerous episode was the invention of antioxidants. More on antioxidants in a moment.
If you’ve ever been mesmerized by a dancing campfire flame, what you were witnessing was a rhythmic and relentless stream of oxidation attacks on the glucose molecules in the wooden log, converting it into charcoal and ash. We have oxygen in our blood, too. Oxygen in our blood can attack things flowing in our blood, including the fatty acids in LDL. After oxygen has attacked the fatty acids in LDL, the LDL particle is said to be oxidized, or basically burnt. Having burnt LDL in your bloodstream is not good.
And this brings us now to the most important question of all:
Question 7) What causes heart attacks and strokes?
Burnt/oxidized LDL in your bloodstream is the cause of heart attacks and strokes. And what oxidizes LDL? Several things, including smoking, emotional stress, and vegetable oil. For references on my vegetable oil claim click here. Remember how earlier I said a particle of LDL is like Uber Eats for your cells? When LDL particles are oxidized, your Uber Eats fat and cholesterol delivery stop working and start having accidents that put their caustic contents in contact with the cells lining your arteries.
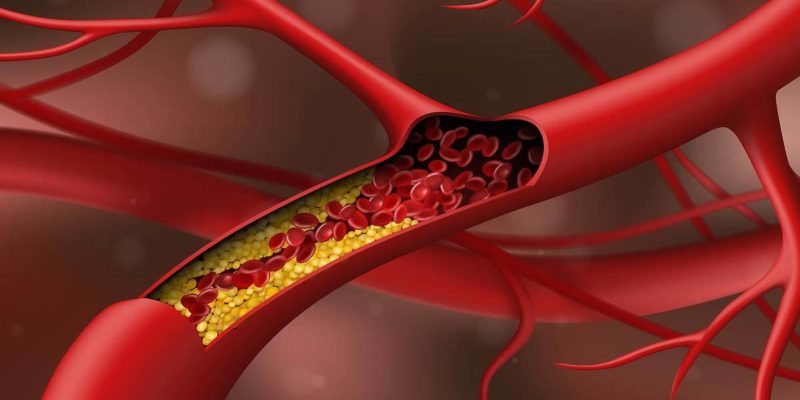
The oxidized fat and cholesterol have toxic effects on those cells. They can cause a kind of wound in your artery that the body attempts to heal. But if your LDL continues to oxidize and your arteries are continually exposed to more and more toxic, oxidized fats and cholesterol, the wound, called a “fatty streak,” never heals and the lesion continues to grow. Eventually, the fatty streak becomes a large plaque, one that can ultimately break up and cause a clot that manifests as a heart attack or a stroke.
The AHA would have you believe that the cause of arterial damage is the cholesterol found in these lesions. In reality, it is the process of oxidation destabilizing the lipoprotein particles that leads to this kind of arterial damage.
Let’s break that down.
LDL GETS OXIDIZED AND THAT’s WHAT DAMAGES ARTERIES
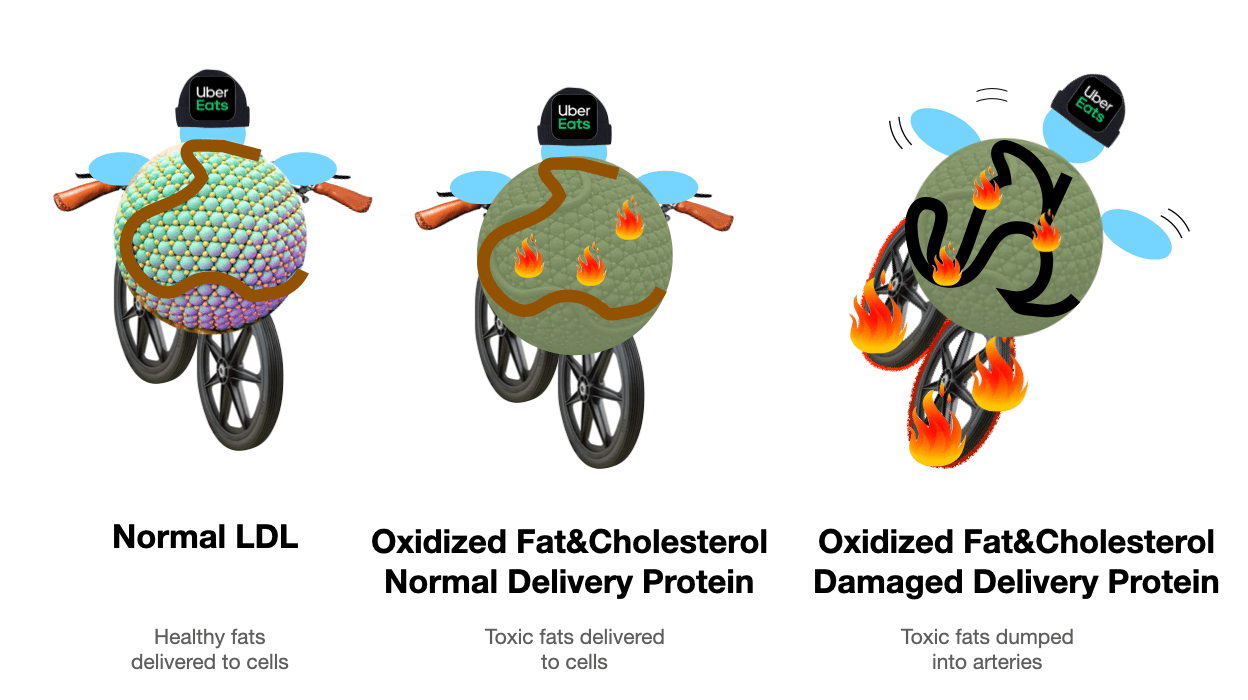
When a particle of LDL is just a little bit oxidized, it’s like the meal you ordered was burnt to a crisp. Instead of a nice tasty pizza, your cells get a box of garbage they have to dispose of. This is not healthy for any of your body’s cells. (It can damage certain large arteries from the outside in, through little capillaries that feed the larger, more muscular arteries like the abdominal aorta.)
When LDL is significantly more oxidized, not only is the food burnt and useless, the delivery vehicle itself is damaged and so unsafe it really shouldn’t be on the road. That damaged vehicle will never make a delivery and eventually will careen out of control, crash and burn on the side of the highway, damaging the cells that line your artery. Over time, the damaged crashed vehicles weaken and scar the artery and ultimately cause thick accumulations of the sticky and greasy contents of the oxidized LDL. If enough of these accidents occur in an artery going to your heart or your brain you can suffer a heart attack or a stroke.
The key to losing fear and learning to love your LDL lies in remembering that only oxidized LDL causes heart attacks and strokes. Regular, healthy LDL does not damage your arteries or build up as fatty plaques. That means no matter how high your LDL, if none of your LDL is oxidized, you won’t get heart attacks or strokes.
And the key to understanding why cholesterol pills are modern snake oil comes from remembering that no matter how low your LDL, if most of it is heavily oxidized, you’re still building up plaques in your arteries and still risking a heart attack or a stroke.
Coming up in this series, you’ll learn how easy it is to become heart attack proof. In the next section, we’ll turn our attention to how your doctor, as wonderful as he or she may be, has been misled by fake science coming from the American Heart Association. Their faith in the AHA is so complete, that it occurs to only a handful of doctors to question the dietary advice they are parroting to their patients.
But what if the AHA were bought and sold decades ago? What if they abandoned science in the name of profit knowing that millions of Americans would die as a result? Could something so sinister be true? Stay tuned for next week’s article to learn the deadly truth that even your doctor doesn’t know.
Source:
Oxidation of LDL particles occurs in a stepwise fashion https://www.researchgate.net/figure/Difference-between-OxLDL-and-MM-LDL-LDL-is-thought-to-be-modified-in-a-stepwise-manner_fig3_51207730
More sources available: https://drcate.com/pufa-project/#atherosclerosis
Ready for Part Two? Click here: https://drcate.com/cholesterol-what-the-american-heart-association-is-hiding-from-you-part-2/
Related Posts

This Post Has 13 Comments
Note: Please do not share personal information with a medical question in our comment section. Comments containing this content will be deleted due to HIPAA regulations.
Hi Dr Cate. Thanks for this great article. I also just finished reading Deep Nutrition and was wondering if your lipid profile interpretation guidelines (i.e. triglycerides < 150 and LDL/HDL < 3) apply to children as well. My daughter (age ~5) has been seeing a cardiologist for her "high cholesterol" but her numbers [just barely] meet the criteria that you say are good. She also has a "high" Lp(a) but I haven't seen you comment on that biomarker before. Appreciate any thoughts you have or resources you can point me to for understanding/managing "high cholesterol" in children. Thanks!
Just a heads up, there is a typo in the sentence, “Severla things, including smoking, emotional stress, and vegetable oil.” You misspelled “several.”
Thanks. This was written before grammarly.
Hi Dr Cate!
Absolutely love your info and brain-food — I’m a pretty healthy keto nut who has been reading different sites on their take on cholesterol, and really appreciate what you’re doing here.
Random/FWIW — Your “Comments containing this content will be deleted due to HIPAA…” notice on your Comments pages (re: personal info in medical questions) should just say ‘Comments with personal information will be deleted due to privacy.’ As a 20-year HIPAA governance IT pro I’ll note that a stranger sharing PHI in a comment here in no way violates HIPAA Treatment / Payment / Ops mandates if you’re not already contracted w/ them. You’ve entered into no contract thus no TPO conditions can exist. You’re not a covered entity if you’ve not consulted them, thus it’s zero HIPAA violation for someone to post their personal info or you or anyone else to read it. Granted, it’s not wise for them to do so, but that’s on them. You’re invoking HIPAA incorrectly — just note ‘for privacy.’ Respectfully submitted. 🙂 Cheers.
Yes that is incorrect and I asked my team to remove such notices but I think that one was missed. Where did you see that, was it an email or on my website? Thank you for your help!
Dr Cate, are you taking appointments ? thank you!
Yes please visit this page for information. https://drcate.com/book-appointment-with-dr-cate/
I would love to have been a fly on the wall when your doc said s/he wasn’t happy with your cholesterol numbers ? …As a layperson, I just get the bum rush ?
But I guess it’s not funny. I know a number of people who gave up processed foods and embraced animal fats only to have their doctor scare them off their new diet with the threat of statins ? It’s hard for average folk to stick to what they’ve learned when their doc says they’re risking their life.
Another fascinating and informative article by Dr. Cate. I have read all of your books and found them to be awesome reads. If your implied theory about the AHA is correct (i believe it is) I think a similar fate has befallen our public health authorities, i.e. USDA, FDA, NIH, WHO, etc. There is so much evidence supporting your views on the “hateful 8” and other data on high carbohydrate diets its unclear how we go up against these formidable organizations (rhetorical). Thanks for sharing this article Dr. Cate.
That’s why it isn’t just about the cholesterol.
But because statins help to reduce fresh cholesterol synthesis, they’re marketed and sold like hotcakes.
While not addressing the issue at all.
Statins don’t even support the elimination of excess cholesterol from the body!
What if you have genetically high LP(a) and calcification in the arteries? What is recommended? Cardiologist says go on a statin or PKS9 inhibitor, but they raise LP(a) and don’t remove plaque.
Great article and very informative. Another factor causing damage to the circulatory endothelial cells (inflammation, lesions, and scar tissue or plaque), that I’ve been researching, is glycation. Any thoughts?
Great start to the series. Just last week I was looking for a good explanation. Dr. Attia’s series is also good but too technical for the people I want to send it to. This is arriving (for me) just in time. Sharing.