Why It Matters That Seed Oils Are Being Recognized as Ultra-Processed The US Dietary Guidelines…
The Truth About Coronary Calcium Tests
Table of Contents
- What A Coronary Calcium Test Can—and Can’t—Tell You About Your Heart Attack Risk
- Failure #1: Not Listening To The Patient’s Symptoms Before Ordering Tests.
- Failure #2: Assuming “Chest Pain” Equals “Heart Problem”
- Failure #3 Using Gastric Reflux as an Excuse to Do Expensive, Invasive Heart Tests
- Failure #4: Not Contextualizing a High Coronary Calcium Score As Probably Normal For Age and Sex
- Failure #5: Not Telling Patients That There Are Different Types of Plaque
- Failure #6: Leading Patients To Believe Statins Can Reduce Coronary Calcium Scores
- Failure # 7: Not Telling Patients That The Body Can Put Calcium In Your Arteries Without Drugs
- Failure #8: Not Clearly Explaining What Having Calcified Plaque and a High CAC score Means
- Failure #9 Not Telling You That Your Body Can Bypass Plaques ON ITS OWN (No stent, no surgery required) With Proper Support From YOU
- Failure #10: Using Stents and Bypasses In Situations Where They Won’t Save Your Life
- Failure #11: Not Telling Patients That Removing Calcium From Plaque Doesn’t Solve Anything
- Failure #12: Leading You To Believe That A Little Bit Of Plaque Inevitably Becomes More
- Failure #13: Not Ordering a Test that Can Show All Three Types of Plaque
- Does He Actually Have Dangerous Plaque?
What A Coronary Calcium Test Can—and Can’t—Tell You About Your Heart Attack Risk
The way most doctors use these tests exemplifies structural failures of the healthcare industry as a whole.
I’ve gotten numerous requests to write an article on coronary calcium tests over the years. Then I met George, whose experience within the medical system finally pushed me to do it. As you’ll see, these tests are widely misused.
But it’s not just that cardiologists misuse the coronary calcium test. The entire system fails to follow protocols I was taught are necessary for proper patient care. The healthcare system now behaves less like a healing profession and more like a self-serving organism, consuming enormous resources while too often harming the very people it exists to serve.
As this story shows, reflexive testing too often substitutes for the more difficult and time-consuming interview process. Diagnoses are never made. Test results are often incompletely shared. Patients are even misled into undergoing invasive procedures that have no chance of helping them. My medical school mentors who taught me how to take a careful history would be rolling in their graves if they knew.
This article is continued below...(scroll down)


It helped. I feel great.
"It’s helped. I feel great."
Kobe Bryant
NBA baskeball player

This has been life changing
"Let me tell you this has been life-changing. I have all of her books, in audible and ebooks! I have gotten rid of all the hateful 8 oils. I have trained my body to eat its own previously toxic body fat. Download that pod it's a game changer!"
Megyn Kelly
Broadcaster / The Megyn Kelly Show

Life changing
Deep Nutrition changed my life.
Jesse Watters
Fox News Primetime host
Saved my life
I would like to thank you for literally saving my life. Back in February, I had to be hospitalized while on vacation in Phoenix with an A1C of 11% and had to start taking 2 types of insulin and 2 other meds. I read the Fatburn Fix in April, and followed the program to a tee, and I’m down by 15 pounds, 6.8 A1C, and only one once weekly diabetes medicine. Prior to reading the book, it was almost impossible for me to lose weight as a diabetic.
Leontyne Tompkins
I feel free
For the last month, I have really been reading all labels on everything. I have completely remove those 8 oils you talk about. I must tell you, I feel great! I have more energy and I am now 197 lbs (have always been around 205 to 210lbs). I eat potatoes with real butter, grass fed steak, pasta with the right toppings. I eat everything! I seem to crave less sugar. I love it!
Robert Kirkendall
I feel so much better
I had terrible aches and pains everywhere in my body, my hands, shoulders and knees. I feel so much better and the way I feel is motivating me every day! Thank you
Mike Deb Wootan Burcin
Better than ever
I am an anesthesiologist in Orlando and a huge fan of both of your books! I have been incorporating your principles for the last 10 months and feel that my health is better than ever.
Marnie Robinson, MD
My allergies disappeared
The biggest difference for me (and a surprising one) is that my allergies have almost completely disappeared! This is a big deal for me, because I’ve had allergies most of my life and they have often affected what I do which is a teaching music in [a public school district]. In general, I feel much better and have more consistent energy throughout the day.
Erica Turrell
Heart Palpitations have Stopped
I’ve lost 20+ pounds (also fasting 16-24 hours daily) and haven’t had palpitations except for one occasion — I had a mini bag of Fritos for the first time in July. And, I feel better now on a daily basis than I ever did all through college.
Mike Wright
Deep Nutrition and Fatburn Fix reader

I’ve lost over 50 pounds
I’ve lost over 50 pounds. I’m 56 years old. Cutting processed food and unhealthy fats from my diet was one of the first things I did on my health recovery journey...I went cold turkey off the bad oils. Emptied my pantry into the trash and just started eating real food
Mitzi Wilkinson Champion
Knowledge I didn’t know I needed
Your Fatburn Fix book is amazing, my friend. Thank you! I’m an Functional Nutritional Therapy Practitioner and I know my stuff. This is the extra layer of knowledge I didn’t know I needed. Well done!
Jennifer Dillman
Fatburn Fix reader
Lost a solid 20 lbs and my bloodwork is great
I have lost a solid 20 lbs and my bloodwork (after 3 months of eating your way) was even better! I was metabolically healthy (per your book) before I read your book, but barely. Lowering my weight, sealed the deal! I have been talking about you and your book to anyone who will listen...Thank you for all you’ve done and what you continue to do! You are changing lives for the better!
Missy Cramer
FatBurn Fix reader
Lost 20 lbs I could never shed
I love your Fatburn Fix! Has helped me so so much! I have had the dreaded weight all my life - 20 or so pounds I could never shed. I have lost that now. I only eat 2 meals a day lunch and dinner with a glass of milk or cappuccino around 4 to hold me over. No snacking and not bad oils. It has been the key to unlocking my fatburn. I work out in the am and believe I am burning fat for energy not from food!
Lauren Smith
I feel great
My waist is four inches smaller. I feel great and many of the minor aches and pains that I had (knees and lower back) are gone. Also, my muscle tone is amazing, even though I have not increased my workout routine.
Richard Janelle
Completed Dr Cate's online course

The go-to for strength and conditioning coaches
Whenever I advise my clients about eating to perform I go straight to what I have learned from Dr. Cate. Her book Deep Nutrition has become the go-to for strength and conditioning coaches across the country.
Kent Matthes
Major League Baseball Agent with WME Sports

Dismantles the lie
Dr. Cate dismantles the lie that seed oils are healthy, which may the biggest lie about nutrition and health because it’s so insidious.
Ken D Berry, MD
Author of Lies My Doctor Told Me

She knows the chemistry
Dr. Cate alerts us to the harms of seed oils and she’s convincing because she knows the chemistry better than anyone.
Dr. Drew Pinskey, MD
Globally recognized internal medicine and addiction medicine specialist, media personality, LoveLine Host, and New York Times bestselling author

No one is better at communicating nutritional truth
Dr. Cate has had the single greatest impact on how we talk to people about fueling for both performance or durability. While we all are a little unique, the foundational principles of human nutrition are immutable. If you are looking to create a more durable, resilient body, no one is better at communicating nutritional truth than Dr. Cate.
Dr. Kelly Starrett
Physiotherapist coach and New York Times and Wall Street Journal bestselling author

Highly recommend The Fatburn Fix
Dr. Shanahan has had a significant impact on my practice of medicine. I am known as a Low Carb Doctor, but I never really appreciated the negative effects of processed seed oils on the health of my patients. I highly recommend The Fatburn Fix to my patients and have a loaner copy in my waiting room. It is amazing how quickly blood sugars and overall health improves with cutting seed oils. It is not just about the carbs!
Dr. Brian Lenkzes, MD
CEO of LowCarbMD San Diego, co-host of Low Carb MD Podcast and host of Life's Best Medicine Podcast

Respected in the sports world
Dr. Cate reordered my diet when I was with the L.A. Lakers, and the benefits, for me personally, were felt immediately and have served me to this day. I’ve come to take real food so seriously I started a small family farm. I know of no M.D./nutritionist more respected in the sports world than Dr. Cate Shanahan.
Chris Kaman
NBA Player

Brought seed oil issue front and center
Cate brought the seed oil issue front and center. Healthy fats matter. So much so that I created an entire product line to swap out bad fats with good.
Mark Sisson
Founding Father of the Primal/Paleo Movement

Optimal health starts with food
If you want to understand how optimal health starts with food, start with Dr. Cate. Her book Deep Nutrition leaves you with an appreciation of the profound relationship between our genes and the planet, inspiring us to be good shepherds of both.
Dallas Hartwig
Attribution author of The Whole 30

Helped me with endurance
Deep Nutrition really helped me with endurance. I started to feel better as a player. I was able to run more, I was able to be more active …and I just decided to keep going with it to this day.
Dwight Howard
NBA Player

Silver bullet for me
Dr Cate’s teachings helped me lose 60 pounds like it was nothing. It was like a silver bullet for me.
Paul Grewal, MD
Dr Grewal Internal Medicine, MD, author of Genius Foods
Radically improve your health…
Dr. Shanahan has provided a solid reference that deserves a place in the library of anyone who is seriously interested in nutrition. Her perspective on the vital role that healthy fat has in our diet is novel and, if implemented, can radically improve your health.
Dr. Joseph Mercola
Author of Fat for Fuel and Founder of Mercola.com

Pull up a chair…
I have based my work on the idea that getting the right kinds of healthy fats into your body and avoiding the worst fats is essential to optimal health. I've interviewed dozens of the world's top experts about this, and I know of no one who speaks more eloquently on this topic than Dr Cate. If she’s talking fats, pull up a chair. Take notes.
Dave Asprey
Author of the Bulletproof Diet
The key to unlocking my fatburn
I love your Fatburn Fix! Has helped me so so much! I have had the dreaded weight all my life - 20 or so pounds I could never shed. I have lost that now. I only eat 2 meals a day lunch and dinner with a glass of milk or cappuccino around 4 to hold me over. No snacking and not bad oils. It has been the key to unlocking my fatburn.
Lauren Smith
Saved my life
I would like to thank you for literally saving my life. Back in February, I had to be hospitalized while on vacation in Phoenix with an A1C of 11% and had to start taking 2 types of insulin and 2 other meds. I read the Fatburn Fix in April, and followed the program to a tee, and I’m down by 15 pounds, 6.8 A1C, and only one once weekly diabetes medicine.
Leontyne Tompkins
> Tears of joy
I'm crying tears of joy and appreciation for all you've done for me and my health! Without Deep Nutrition and Fatburn Fix, I would literally still be in the vicious cycle I'd been fighting all my life! In a nutshell - I am no longer a compulsive overeating addict suffering under the crushing 'thumb' of all food and alcohol.
Penni Wicks
I wrote this article not to curse the darkness, but to light a candle–and empower you to protect yourself.
Failure #1: Not Listening To The Patient’s Symptoms Before Ordering Tests.
This story focuses on a man named George, who kindly gave me permission to tell his story here.
Back in 2018, George developed pain in his calves. It bothered him enough to go to his doctor. So off he went.
When you go to a doctor with a symptom, the doctor is supposed to ask a bunch of diagnostic questions. These would include questions like “What brings on the pain?” “How long does the pain last?” “What do you do to relieve the pain?” But when I spoke to George years later, he was pretty sure his doctor didn’t ask those kinds of questions.
Instead, his doctor focused on just one possibility, a circulatory problem called intermittent claudication. Intermittent claudication is caused by blockages in the arteries to the legs that limit blood delivery. It can be very serious. So physicians are supposed to ask people about their symptoms to see if the pattern fits. We can easily find out with two questions:
- Does pain start while walking?
- Does it go away when you stop walking, or sit?
If the answers to both are no, then there is at most a very low chance that the patient has claudication. The range is 0-10%, and the doctor should move on to consider other conditions.
On the other hand, if the answer to either one of those two questions is yes, then it could be claudication, and testing needs to be done.
The Rollercoaster Ride Begins…
When I asked George if he’d had claudication symptoms, he said definitely not. Meaning there was no need for further heart testing. In other words, if the very first doctor he saw had been more thorough, it could have saved George the many years of worry I’m about to describe in the rest of his story.
So even though there was no real reason to send him for a test for intermittent claudication, his doctor sent him anyway. When George returned to review his results, they were normal. So what caused the leg pain? His doctor didn’t pursue it further. Fortunately, his leg pain would later go away on its own.
Unfortunately, while at the office to find out his first set of results was perfectly normal, his doctor asked him another question. Not about his leg pain, which remains a mystery to this day. But about symptoms George was not the least bit concerned about. As you’ll see, that exchange has since launched George into years of treatments, unnecessary prescriptions, and follow-up visits.
Failure #2: Assuming “Chest Pain” Equals “Heart Problem”
Back at the doctor’s office, after George found out the results of his leg scan were normal, his doctor asked if he ever had chest pain.
George told me, “Not knowing what kind of chest pain he was referring to, I said yes.” George had acid reflux, which can also cause chest pain. Chest pain from acid reflux is often very easy to distinguish from chest pain from a heart problem. But a doctor has to ask the right questions to know the difference.
During my conversation with George, I asked him if he remembers the cardiologist asking diagnostic questions like “Is your pain brought on by overeating?” and “Does exercise bring it on?” and “Is it relieved by rest?” George remembers being surprised by the lack of clarifying questions. Instead, the primary doctor jumped right to the conclusion that it could be his heart, and sent him to the cardiologist.
Unfortunately, the cardiologist didn’t do a diagnostic rundown, either. However, he was happy to order a bunch of tests.
Failure #3 Using Gastric Reflux as an Excuse to Do Expensive, Invasive Heart Tests
The minute George set foot in the cardiologist’s office, any semblance of diagnostic decency flew out the window. Rather than first determining whether George’s symptoms were even compatible with heart disease, the cardiologist immediately ordered an EKG. Then, an exercise stress test, a CT scan, and finally a nuclear stress test. To me, this is a classic fishing expedition: ordering multiple expensive tests before establishing that there’s a good clinical reason to suspect the disease you’re looking for.
An excuse I frequently hear for ordering tests that aren’t medically indicated is this:
“Better safe than sorry.”
It sounds reasonable, but it ignores a fundamental principle of medicine: every test should answer a question that genuinely needs answering. Tests aren’t harmless. Some expose patients to radiation or invasive procedures; others lead to false positives and unnecessary follow-up. All consume time, money, and attention.
On a more basic level, this practice defies common sense. Because if you haven’t done a basic history, you’re putting the cart before the horse. And putting your patients’ lives at risk.
In George’s case, his doctors should have established whether any of his symptoms actually suggested heart disease before ordering so many heart tests.
Fortunately for George, none of these tests revealed significant blockages. Even though there were no significant blockages, the CT scan showed calcium in the arteries to his heart. Quite a bit. His coronary calcium score was 904 on a scale that starts with 0. That sounds pretty high, right? Well yes, but…. the score can be as high as 5000, and it’s very age dependent. Which leads us to the next failure.
Failure #4: Not Contextualizing a High Coronary Calcium Score As Probably Normal For Age and Sex
Patients like George who come to me concerned about their high scores, and are over 40 years old, have generally been led to believe that their high score is more unusual than it really is. One very disturbing thing that I’ve noticed about some of these reports is that they do not provide you—or your doctor—with one vital piece of information: what number is considered abnormal for your age and sex?
George’s report was typical in that it contained this alarming language: “A calcium score of 401 or higher indicates extensive plaque with a high likelihood of coronary narrowing.” That sounds frightening, especially if your score is much higher than 401. But there’s an important problem with using that number as a universal benchmark. It comes from studies of people who had much higher chance of having heart disease than George. For example, they’d had previous heart attacks, or were diabetics, or had chest pain with exercise. George wasn’t in that situation. It’s like he was an orange being compared to an apple and then told he had abnormally lumpy skin.
How Coronary Calcium Scores (CAC scores) SHOULD Be Reported
The range of possible coronary calcium scores is wide, starting at 0 and going up over 5000. It tends to go up as we age. The report tells you how far you’re above or below your age-matched average.
But for tests like the CAC score (BTW, CAC stands for coronary artery calcium), simply being above average for your age doesn’t equate to abnormal. In this scenario, a result usually has to fall well outside the normal range—often about two standard deviations from the mean—before physicians should regard it as clearly abnormal. To be considered truly unusual for his age, George’s score would have needed to be over 1609, not 904. The report should reflect that. But it doesn’t.
So as you can see, the report itself is somewhat misleading, but that’s actually a minor issue compared with the deeper problem of CAC testing. It tells you how much calcified plaque you have, but it doesn’t tell you whether you have the kind of plaque that’s most likely to cause a heart attack. To understand this limitation of CAC testing, you need to know that there are several different kinds of plaque with very different consequences for your health.
Which takes us to the next failure:
Failure #5: Not Telling Patients That There Are Different Types of Plaque
Most patients who’ve been advised to get a coronary calcium test are generally under the impression that plaque is plaque. They know you can have different amounts of plaque, but they’ve not been told that there are different types of plaque. This is vital to know because different plaques have completely different impacts on your health.
In reality, there are three types of plaque. Two are very common: stable (or calcified) and unstable (or fatty). A third is less common and also the most dangerous: inflammatory. All plaque starts out fatty and soft—and a little unstable. This kind of fat is potentially dangerous because it is at risk for becoming inflamed. When it becomes inflamed, it is truly dangerous becuase is at great risk for rupturing, which often causes heart attacks.
But the body is smart. Incredibly, it’s got a treatment plan for hardening these softer, potentially dangerous plaques. The body adds calcium and protein to the fat, stabilizing and hardening it. So even though you may have plaque, which sounds bad, if it’s calcified, your body has addressed the issue in the best possible way.
Three Major Types of Plaque: Fatty, Calcified & Inflamed

I hope you can see where I’m going with this discussion. As you may be guessing, since it’s called a Coronary Calcium test, the CAC test can only see the plaques that have calcium. It can’t see plaques that are fatty or inflamed. So a high calcium score tells you only that you have a lot of stable, not very dangerous plaques. What it doesn’t tell you is whether or not you also have the potentially dangerous fatty plaques. Nor does it tell you whether or not you have any of the most dangerous, inflammatory plaques.
The thing is, we now have a test that DOES show all three types of plaque! And people should be told about this test. I’ll discuss it below.
Instead of being told the truth about plaque, or that there is a better test, most people are told to take a statin. Including George.
Failure #6: Leading Patients To Believe Statins Can Reduce Coronary Calcium Scores
After George’s doctor told him about that score of 904, he prescribed George a statin to keep his cholesterol down. George recalls his doctor saying that without a statin, his plaque could break off and cause a heart attack. So of course, with that scary image placed in his mind, he started a statin. He was under the impression that taking a statin was going to help reduce his calcium score, thus reversing the atherosclerotic plaque in his arteries. He dutifully took the statin for two years, and then in 2020 requested another CAC test to see if the score had changed.
It changed, alright. But not the way George was expecting. The second score was 1170—hundreds of points higher. The doctor explained this disappointing result as follows: “because the Pravastatin is causing more calcium to stick in your arteries.”
That statement is one of those little lies that drives me crazy. Statins don’t cause calcium to stick in your arteries. The body does that magic act on its own. If statins do anything at all, they may reduce the development of new fatty plaques by reducing the amount of easily oxidizable triglyceride in the blood. But a more effective and safer way to reduce the development of new plaques is through diet. (If you’d like to learn more about when I’d recommend statins, LMK in the comments).
A conscientious physician should tell people that statins will make their score go up instead of allowing them to believe otherwise.
But few doctors do that. Probably because something in their mind warns them that if they give their patients this counterintuitive information, the patient might start asking pesky questions.
Which leads me to the next failure.
Failure # 7: Not Telling Patients That The Body Can Put Calcium In Your Arteries Without Drugs
As I mentioned above, the body puts calcium in our arteries all the time. That’s how calcified plaque forms. That’s what causes high CAC test scores. We don’t need drugs for that. Period.
As the body adds calcium to a fatty plaque, it also adds protein, which provides the matrix that supports the calcium (see figure above). At the same time, much of the soft fat is removed. A little cholesterol remains behind, providing waterproofing and serving as part of the plaque’s structure. As plaque changes from fatty to stabilized, it often shrinks somewhat. This observation has been used to suggest that statins shrink plaque. But the real story is that plaque stabilization and shrinkage are both part of the body’s natural healing process. No statins required—if you follow a lifestyle that allows our healing processes to play out.
So I hope you can see that the simple story George was told is already starting to unravel.
Those questions bring me to Failure #8.
Failure #8: Not Clearly Explaining What Having Calcified Plaque and a High CAC score Means
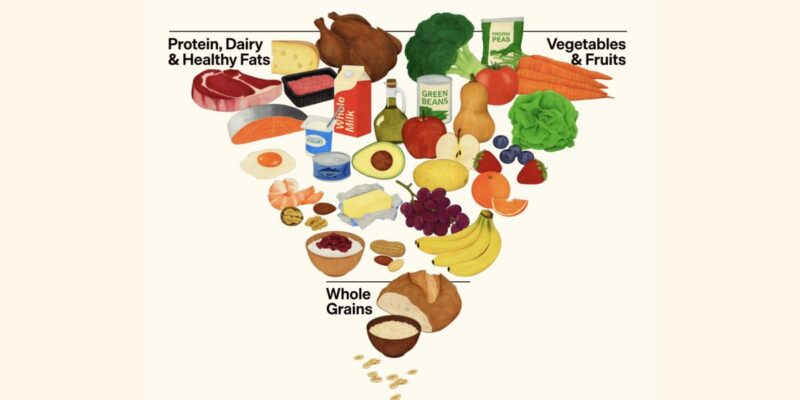
After I told George the good news, that his calcified plaque is unlikely to cause a heart attack, I had to give him some bad news. The fact that he has calcified plaque means two things. First, that his prior diet had harmed his arteries. His prior diet was high in seed oils and low in protein–two factors that promote oxidative stress and atherosclerosis. Second, anyone with calcified plaque is statistically more likely to have fatty plaque somewhere in their arteries. Fortunately for George, his improved diet probably prevented that—and we now have a way of testing this idea (discussed below).
But the most important thing to know about calcified plaque is that it can block off little tiny arteries. Large coronary arteries give rise to countless tiny branches. These tiny branches dive deep into the heart muscle to supply it with blood. Long before there’s enough plaque to clog the big arteries, there’s often more than enough to clog the little tiny ones. And in this case, it doesn’t matter whether the plaque is fatty or calcified. These occlusions reduce blood flow to the muscle downstream of that tiny artery.
If the body is unable to compensate for this loss of blood flow, that little portion of heart muscle can be damaged. Many such blockages can cause structural changes that make the heart stiff, weak, or both. This condition is called heart failure.
Fortunately, your body has a remarkable backup system for this problem of little blockages that can prevent this from happening.
And now we need to talk about what may be the biggest medical failure of all:
Failure #9 Not Telling You That Your Body Can Bypass Plaques ON ITS OWN (No stent, no surgery required) With Proper Support From YOU
Most non-medical people are led to believe there are only two ways to manage a blocked coronary artery: stents or bypass surgery. That’s not true. Your body has been building its own bypasses your entire life.
This remarkable process is called angiogenesis, meaning the formation of new blood vessels. It’s how your body grows, heals injuries, adapts to exercise, and responds to gradually developing coronary artery disease.
As described above, when plaque slowly accumulates inside a coronary artery, it gradually narrows or obstructs the openings of the tiny branches that supply blood to the heart muscle. Because this process usually unfolds over many months or years, the body has time to adapt. It does so by growing brand new baby blood vessels, called collateral vessels. These tiny collateral vessels can deliver oxygen and nutrients to the heart muscle just as well as the originals did. In fact, people who are really good at growing collateral blood vessels can have a completely blocked major artery and still have completely normal blood flow to their heart.
It’s all about the speed at which a new blockage develops.
If an inflammatory plaque suddenly ruptures and causes a heart attack, blood flow is cut off in minutes. There isn’t enough time for the body to build new vessels. That is why emergency procedures such as stents or bypass surgery can save heart muscle—and save lives.
Stable, calcified plaque is different. It develops gradually, giving the body its opportunity to compensate by building new blood vessels. But not everyone’s body can compensate.
Whether your body builds new blood vessels depends on your physiology.
Growing new blood vessels is an energy-intensive repair process that depends on healthy blood vessels and healthy signaling between cells. Smoking, physical inactivity, diabetes, poor nutrition, and other factors that damage the lining of blood vessels can impair this remarkable ability.
At this point, I should give you a little more of George’s background. George had always taken his health seriously. He didn’t smoke, exercised regularly, and for several years had been following the dietary program I recommend. His second stress test, a nuclear exercise stress test, showed normal blood flow throughout his heart during exercise. In other words, despite having calcified plaque, his heart appeared to be getting all the blood it needed.
Unfortunately, because most patients don’t know that this natural bypass system exists, they also don’t know that not every blockage seen on an angiogram requires a stent or bypass surgery, as I’ll discuss next.
Failure #10: Using Stents and Bypasses In Situations Where They Won’t Save Your Life
Cardiologists know about your body’s ability to bypass itself by growing new blood vessels. But their patients usually don’t. And this makes it all too easy to sell unnecessary procedures. Most people assume that seeing a severe blockage on an angiogram automatically means it needs to be opened with a stent or bypass surgery.
But the truth is, having a blockage does not always mean you need a stent. In fact, studies show that putting stents into people with stable plaque and stable symptoms does not save lives. It may reduce their symptoms. But it’s not a life-or-death thing. Unfortunately, my patients who’ve gotten stents in this scenario were not told the truth.
According to numerous investigations, including one by USA Today, unnecessary coronary procedures remain a significant problem. These procedures are generally not performed on people with completely normal arteries. They are performed on people who have visible blockages on angiograms. If patients don’t understand the difference between a blockage that requires treatment and one that does not, they are in no position to question the recommendation.
Another survey reported on in this video, found that a substantial percentage of cardiologists acknowledged performing procedures they believed were unlikely to benefit the patient. Regardless of the reasons, this is exactly why patients deserve to understand how coronary artery disease really works before deciding whether an invasive procedure is necessary.
Failure #11: Not Telling Patients That Removing Calcium From Plaque Doesn’t Solve Anything
A lot of people, including George, have asked me, “How do I get the calcium out of my arteries?” My answer is always the same: You definitely don’t want to do that.
Once plaque is stabilized, it’s as durable and waterproof as cured bathroom tile caulk. I’ve examined plaques removed from carotid arteries back in the day when carotid endarterectomy was commonly performed. They are remarkably tough.
George left his cardiology appointments believing that the calcified plaque in his arteries could break off and kill him. I’ve heard the same concern from many patients over the years. But having a lot of calcified plaque does not, by itself, mean that some area of plaque is more likely to rupture. The danger comes from inflammatory plaque.
Failure #12: Leading You To Believe That A Little Bit Of Plaque Inevitably Becomes More
Let’s look at the picture almost every cardiologist’s office has hanging on the wall for patients to see.
Typical Misleading Model of Coronary Artery Plaque Progression

This picture is very misleading. It doesn’t show the calcification process at all, leading people to believe there is only one type of plaque and it’s dangerous. That’s not true–as we’ve discussed. This kind of image also gives the impression that heart attacks mainly occur in very large plaques. Also not true. Most heart attacks arise from much smaller plaques, and more than half occur in areas of narrowing so small they are completely invisible on conventional angiograms. And, the picture leads us to believe that, once plaque starts, it’s inevitably going to keep building up. Unless, of course, you take a statin or get a stent. But of course that’s not true either. A healthy diet prevents plaque from building up.
I could keep going all day with these failures because there are many more. But I’ll finish with one last failure—the one George is currently most frustrated by.
Failure #13: Not Ordering a Test that Can Show All Three Types of Plaque
Cardiologists know about all three types of plaque: stable, fatty, and inflammatory. They know a coronary calcium test shows only the stable, calcified plaques. But what very few cardiologists seem to know—at least as of the date I’m writing this article—is that there is now a test that can show all three types of plaque.
George wanted to meet privately becuase he’d attended my master class where I teach about a new type of technology. It’s called Coronary Computed Tomography Angiography (CCTA) and Artificial Intelligence Quantitative Computed Tomography (AI-QCT). Basically, all that means is it’s an AI-assisted CAT scan of your coronary arteries. Two brand names are Cleerly and Heartflow.
These new tests can identify all three major types of plaque, and can be extremely valuable for someone with a high CAC score or a high LDL who is being told to take a statin, change their diet or just trying to understand their true heart attack risk. They’re more invasive than a simple coronary calcium test because they require IV contrast dye. George wanted to speak with me to make sure he understood the science correctly. It was during that visit that I encouraged him to ask his cardiologist for one of these scans. So he did.
The cardiologist’s response surprised both of us.
His cardiologist told him he had never heard of such a thing. He also said the results wouldn’t change his recommendation—which was to take a statin. Therefore, he wasn’t willing to order it.
Do I think George absolutely needs one of these scans? Probably not. But after spending nearly eight years believing his calcium score meant he was living with a ticking time bomb, I think he deserves the opportunity to answer the question that has worried him all this time:
Does He Actually Have Dangerous Plaque?
In my opinion, that’s the question his medical team should have been trying to answer from the beginning.
And in my opinion, George is very unlikely to have dangerous plaques. I say this because of 1) the healthy dietary changes he has maintained since reading my books years ago, 2) his ability to do heavy activity, 3) his lack of diabetes, hypertension, or other diseases that indicate overall high risk, and 4) his normal exercise stress tests. So, in that sense, this story does have a happy ending. Not thanks to his doctors. Thanks to him being proactive about his health.
George’s story isn’t unique. I’ve now heard versions of it from far too many people. When I graduated, the healthcare system wasn’t perfect, but in general we patched people up and sent them on their way better than they came in. Today, it’s become a dangerous maze.
The Medical Labyrinth
That’s what I call the system that converts healthy people into patients.
George’s story began with a minor pain in his calves. Instead of getting a diagnosis for his pain, George got a one-way ticket to enter the medical labyrinth.
George spent the better part of eight years being repeatedly told he had a dangerously high coronary calcium score without anyone explaining what that score actually meant. He was never taught the difference between stable plaque and unstable plaque. He wasn’t told that calcification is part of the body’s natural stabilization process. He wasn’t told that his body can often compensate for slowly developing plaque by growing new blood vessels. He was given a statin, which made him feel sluggish and unhealthy. And when he finally asked for a test that could distinguish among all three types of plaque, he was told no.
Fortunately, George has become proactive about his health. Years ago, after reading my books, he developed the confidence he needed to stop his statin. He also ditched the diet that caused plaque to build up in the first place. At 76 he’s feeling strong and still playing competitive racquetball twice a week, walking 2+ miles a day, mowing an acre with a push mower, and horseback riding. If he hadn’t made these changes, it’s likely that by now another symptom would have lured him deeper into the labyrinth.
I hope that, after reading this article, you now understand coronary artery disease more completely. And I hope this deeper understanding helps keep you, or someone you know, out of the medical labyrinth. If you liked this article, please share. And if you’d like to learn more from me, check out my books and my masterclass.
Now I’d like to hear from you.
Do you think I’m being unfair in calling out these failures?
Have you had an experience similar to George’s?
Would you want a Cleerly or Heartflow scan if you were in this situation, or would you trust your body?
Have you had a Cleerly or Heartflow scan? Tell me below in the comments—I’d love to hear your thoughts.
Related Posts


This Post Has 37 Comments
Note: Please do not share personal information with a medical question in our comment section. Comments containing this content will be deleted due to HIPAA regulations.
A timely post for me as I’ve recently taken that roller coaster ride. And while all the doctors and caregivers were great, I felt like a number on an assembly line passing each specialist for another opinion. I had all kinds of tests which in the end identified a small calcified plaque deposit in my heart. Nothing to worry about no blood flow impedance, no evidence of any activity that would’ve caused blood clots. And now while my cholesterol is in great shape, I believe in part to following dietary arguments presented in your publications, I have been prescribed cholesterol lowering meds(not statin) to ensure that plaque in my heart does not grow. I addition I seem now to have a virally induced auto-immune disease which probably caused my various ailments. So now more appointments with new doctors as I continue on down the assembly line.
Your recent article (and the books and posts) gives me confidence we can care for our health by managing our diets and behaviors. My recent medical experience has left me a doubter. My confidence in health care would be much improved if one person followed me through the whole experience and presented a digestible interpretation.
Thanks for all the work you’ve shared with us.
Great read from skinnylegsandall
My PCP had me get ct cardiac calcium score because my total cholesterol was 249 (high) at my annual checkup. I was not experiencing any problems.
The Agatston total coronary artery score was 1462. lm 0, lad 283, lcx 1179, RCA 0 pda 0. My doctor prescribed 10 mg Rosuvastatin and referred me to a cardiologist.
The cardiologist scheduled a stress test. About a week or two before the the stress test I stopped Rosuvastatin because I felt like I had been in a train wreck, and my muscles wouldn’t move. The exercise mycardial perfusion spect imaging stress test was continuous for 12min, 51 sec. to stage 5 of the Bruce protocol. Heart rate rose from 65bpm to 171bpm which was 112% above predicted maximum. The resting ECG showed sinus rhythm, no significant ST or T wave changes with stress. PVCs occurred during stress but did not persist into recovery. Conclusion Normal hemodynamic and ECG stress test . Gated perfusion images show normal left ventricular regional wall motion with an EF of 64%.
My lab work at that time showed total cholesterol of 228, but my glucose had doubled from 85 to 154!!!!!
That’s when I read Dark Oils and cut out seed oils. I also had to get a continuous glucose monitor to battle the high glucose. It’s a problem that could have been avoided if I just skipped my annual checkups.
Thank you for sharing your story. It made me think about a phrase that doctors used to say a lot, “Worried well.” We used it when people had minor symptoms that were nothing to worry about, like occasionally forgetting where we put our car keys and asking if it could be Alzheimers. We called the treatment “reassurance,” meaning just explaining that it’s not Alzheimers and why not. Unfortunately, now doctors are playing the reverse role. We worry our well patients and provide them with fear rather than reasurrance!
Hi Dr. Cate, I think you’re amazing and I follow you. I love your efforts to share with others about the harm of seed oils. I read some of this article and I do have a question my cholesterol is. Total 225, HDL 73, LDL 132, non HDL cholesterol 152, with a ratio of 3.1 and my triglycerides are 92. I had a calcium score done almost a year ago and it was 0. My father passed away of serious coronary artery disease at the age of 81 having had a second heart attack and already a bypass in his mid 60s and a stent put in at 75- he was taking care of my beloved mother with Alzheimer’s who recently passed at 85. My brother has a higher calcium score. I’m not quite sure what it is. I do take red yeast rice nightly 1200 mg’s, which has brought my cholesterol down from 250 ish. Many doctors have wanted to put me on Stantons but I refuse. Do you recommend I take Stantons based on my information or continue on the red yeast rice? Also, one other quick question: I try to avoid the hateful eight seed oils at all cost, but sometimes difficult when traveling and out to dinner with my husband to his favorite restaurants. There is no seed oils in my home. I never use them for cooking. I also try not to put them on my skin. I wonder what you think about that -is it OK to put on your skin? Some of those sunflower oils are everywhere in Skincare. I try to put on my largest organ similar to what I put in my body. I try to avoid them and use tallow but I wanted your opinion because I go out of my way to not purchase them and it is mind-boggling looking at all the ingredients ha ha! Thanks for all you do and God bless you. <3
Good for you for making all those positive changes!
Thank you for this article! It was very timely for me. I have what my doctor considers high LDL and recommended a statin which I refused, thanks to you! I refused because I also have a very high HDL, low triglycerides, exercise regularly, non-smoker and no history of heart disease. I have cut out all seed oils and decreased my sugar intake. I was thinking of asking for a CAC test but thanks to this article I learned it won’t tell the full story. Thanks for all you do to keep us healthy and to tell us the truth!
I would like to know more about statins please. I have so many questions regarding them. Damned if I don’t take them, damned if I do- but maybe it’s the “safer” route if I do?
Hi Dr Cate
Thanks for the insightful article. I am a huge fan.
You may recall I have high LDL 150 with an ApoB of 112 , HDL 56 , Triglycerides 65. my Oxidised LDL score was in the normal range. 1) oxidised LDL was in the range 56 range <60 U/L
2) LDL Pattern is optimal A
3) HDL Large is 7230 optimal
4) LDL peak size 2180moderate
However the Lipoprotein fractionation was out of range:
LDL Particle number 2045
LDL small 377
LDL medium 504
I am in my late 50's active , work out regularly, eat clean,well etc. I had a CT Angio 3 years ago and my Calcium score was 125 and we spoken then
I was told 20 years to start a statin ( I havent yet) and have tried to manage my diet and lifestyle. The LDL went up from 120 to 150 after my 50's. I struggle in my mind re starting a statin or not as the diet has not been able to bring down the LDL number and ApoB unless i try to eliminate all Fat which i am hesitant to do.
Now besides statins there are PCSK9 inhibitors which are costlier injections but apparently don't have the side effects of the statins. Any suggestions, insights would be most welcome to improve the quality of the LDL Particles and reducing LDL. ApoB?
Many thanks
These are great questions–for a future (probably distant future) post on particle counts.
This was very interesting to me.
I had the Test done because I had two episodes where I felt pressure around my whole chest and into my jaw. My Primary NP ordered the test.
I am 75 – walk 3 miles almost everyday – but am recovering from a broken wrist – and the surgery that put me back together seemed to have compressed nerves ulnar and carpal – I was having all kinds of pain everywhere.
My score is 217, “which places the patient in the 50-75th percentile for asymptomatic, apparently healthy persons of the same age and gender”
I have high cholesterol (287) but I have always had high cholesterol – my HDL is 74 – 87, Trigs are 96, VLDL is 19 – my Primary wants to me to take statins but I refuse – seen too many people suffer from them.
So.. I really appreciate this article.
Thank you so very much!
Toni
Hey Dr Cate, great article as always, and yes,’please keep questioning the modern medical profession! This is also incredibly timely: I’ve just started the numbers game with my doctor, as having had LP(a) and ApoB results come back on the high side, together with higher cholesterol numbers. When I told my doctor I would look at dietary and lifestyle interventions before I consider medication, he looked at me and said “why bother?’ You won’t stick to it, and since your LP(a) show moderate risk, it’s pointless anyway”. Talk about red rag to a bull! So I’ve started reading about lowering what I can lower (ApoB and cholesterol), and found this space is confusing and contradictory. Eat high fat, no! lower saturated fat and eat more vegetables….aargh this all drives me nuts. I’ll reread Deep Nutrition and Dark Calories I think.
Keep up the great work, and yes I would be intrigued to know under what circumstances you would subscribe statins!
Cheers!
The new CAT scans that show all types of plaque require contrast. My UCLA Health kidney transplant docs tell me no contrast for a CT as it could damage the transplanted kidney. Are you aware of a contrast for these tests that is safe for transplanted kidneys?
I read your first edition of Deep Nutrition and have been avoiding the hatefull eight. A combination of what I have learned from you and other sources and my UCLA Health docs I made it to 80 and 25.5 years with the kidney transplant.
Thank You, Robert
Yes, I would like to know the circumstances you would recommend a statin.
Dr. Cate,
This is EXACTLY where my wife finds herself in consultation with her cardiologist currently.
Recent CAC of 500, up from 209 last year.
Family history of heart attack, but she is a 69 y.o. female, regular exercise, ideal body weight, very low- carb diet for 5 years. Triglyceride/ HDL ratio of 0.44!
Hscrp score extremely low.
Of course she has been advised previously to take statins but has not. Now with the new CAC elevation he has advised Repatha.
Good news is that a CCTA has been scheduled in 2 weeks.
Hope to follow up with you after. Any encouragement for her now is appreciated.
Thank you for this superb article!
Sounds like this is a very important fork in the road for you and your wife. Also, and maybe you know this, but CCTA is only the first piece of the puzzle. It gets you the image. The image needs to be analyzed by an AI type technology. That technology (ie Heartflow or Cleerly) can tell you the type of plaque.
Thank you, Dr. Cate. As I understand it her CCTA is Cleerly.
I will report!
The amount of mis/lack of information from practicing doctors is alarming. We need doctors like Dr. Cate to give us the facts. A friend had told me about the CAC test after my primary dr. was harping on me needing statins, with a total cholesterol score of 250. I was refusing the statins and then asked for the CAC test. He said, “No, I will not order it since you would refuse statins even if the score were high.”
After that I read more about the CAC test and decided I didn’t want it anyway. I think a huge health crisis is coming with the amount of people on statins, it is disturbing. It takes an assertive/informed patient to question “the doctor”, and most people are not this way. Thank you Dr. Cate, I am finding all your articles very informative. (I do have a new primary care doctor)
Thank you Dr Cate
When is your next book coming out?
Hi Dr. Cate,
I am 81, and I have a calcium score of 98, which isn’t bad, but it is all in the LAD. My recent lipid profile shows: total cholesterol is 217, my LDL is 129, my HDL is 78, my triglycerides are 59, and my VLDL cholesterol is 10. My LDL and total cholesterol have regularly been high, but so has the cholesterol of my sisters. I don’t have high ApoB. Because of my high cholesterol, my cardiologist has been wanting me to take a statin, but I have microscopic colitis, so that is contraindicated. He has prescribed a PCSK9 inhibitor for me because it bypasses the gut. Because of my calcium score and the plaque being all in the LAD, I asked to get a Coronary Computed Tomography Angiography (CCTA). Apparently I think I have some of the inflamed plaque in my LAD. Even though my doctor explained the results to me, I don’t understand them.
The summary from the Cleerly Coronary Computed Tomography Angiography (CCTA) says:
Atherosclerosis: 76 mm3 Total Plaque (0.1 mm3 Low-Density-non-calcified, 38.7 mm3 Non-calcified, 37.2 mm3 calcified)
Stenosis: 2 Moderate (pLAD, D1); 2 Minimal (pRCA,LM)
Dominance: Right-Dominant
Exclusions: none (100% of coronary -arteries > 1.5mm in diameter were evaluated)
I then got a ffrct fractional flow reserve based on the Coronary Computed Tomography Angiography (CCTA)
Narrative & Impression:
Interpretation: The 50% stenosis in the proximal LAD has a low likelihood of lesion-specific ischemia. The 50% stenosis in the proximal first diagonal artery has a low likelihood of lesion-specific ischemia.
More of my statistics:
I have microscopic colitis, so I have intestinal inflammation
My recent hs CRP is .5
My A1c is 5.6
I’ve never smoked
I kdon’t drink alcohol
I am thin
My blood pressure is good
My Lp(a) is low
My ApoB was 104 when I was tested at the end of 2024
I exercise daily
My diet has been good for most of my life
I’m trying to figure out why I have coronary artery disease.
I would rather not take the PCSK9 inhibitor, but I will if I have to.
Dr. Cate, can you help me figure this out?
Thank you! -Mary Graydon Fontana
Absolutely and I would love to help you. Please visit here to learn how to work with me: https://drcate.com/book-appointment-with-dr-cate/
I signed up for your Master class as soon as I was sent your email and then never heard another word. Absolutely no reply when it said I would.
Also, where can you have this heart test done if Cardiologist don’t want to do them. Someone must be ordering them for patients to have this test done. Thank you.
Thanks for letting me know! I just checked an my program sent it to you. So that means it may have ended up in spam, which sometimes happens periodically even though you’re getting my newsletters…Just to make life fun! To prevent that, you may need to add the email I sent this newsletter from to your email programs list of preferred or accepted senders.
To my knowledge there’s no place yet to get without a doctor’s order. Hopefully soon.
Hello Dr. Cate, Your article was amazingly timely for me, who just received my CAC score last week. Question: Would you agree that in regard to diet, is removing the Hateful Eight the primary goal, or are there other equally important things to pay attention to?
Yes. That alone will get you 80% of the way there. Unless you have a major sweet tooth, then you may need to pay attention to total carbs, too!
I so appreciate your articles… I do not have this issue but I am a very healthy 56 years young women and am just trying to take in all the info I can. Like you said, doctors just push and push for tests as routine even without any symptoms. I would definitely want the test to determine which type of the 3 plaques! To this date I am not on any prescribed medicines…. have read ALL your books! Hoping to keep thriving. 🙂 Thank you!
?? Thank you and happy to hear it! Stay young
It was a great article. I believe you should go on pointing out the inadequacies of the health system. People need to know. I had a CAC test done in 2023. I was referred to a cardiologist but decided not to go. My cholesterol is high because I follow your way of eating. Something I warned my primary care Doc about. He keeps prescribing a statin but I gently refuse to take it. I am continuing to eat properly. I finally gave up french fries for good, lol. I would like to get the CCTA test, but only for my own information. I hope this is what you were asking for and I tried to leave out precise details.
Thank you, Judy. Stay strong!
Please letme know when you think we should be given statins as a result of a high CAC (heart calcium) CT scan result. Thank you!
Been following Dr. Cate since I heard her on Catholic Radio almost two years ago. I read Dark Calories, which more than taxed my chemistry and biology understanding from high school (in the 1970s). I have also read several other books on the same basic subject from Dr. Means and others. My frustration is now that basically none of the doctors I see know anything about any of this! I do have a BS degree, but it’s in business; the college level “science” I took was geology aka “rocks for jocks”. How is it that an almost 70 year old retired loan officer now knows more about this subject than the majority of the doctors practicing today? Or am I wrong about this?
No, not at all unfair, we need more Drs like you. I, too, read one of your books, Deep Nutrition. I liked it so much and found it so easy to read, I bought several copies and gave them to family members I deeply care about and wanted to share the wealth of information you gave in a very well written manner.
I’m looking for a Dr like you in the Phoenix area. One of mine didn’t even know what autophagy is. Lol, we are all in trouble and need to head your advice on diet and exercise. Keep up the good work.
Would love to read your opinion on statins, the whys and why nots. I have high cholesterol and my doctors have been telling me for years to medicate. I am unconvinced. This is a great article about the CAC #’s and how to evaluate! Thank you! N
Wow, Dr. Shanahan does this hit home. In 2016 a “lipid specialist” ordered a CAC for me after the results of an NMR cholesterol test. The CAC scores were not good, not outrageously high but I think in the 400-500 range. He wanted to immediately put me on a statin. I told him I would have to research the drug before taking it. He all but said I should get my affairs in order. My wife said I was white as a ghost when I got home. I didn’t take the statin and wouldn’t ever. I resumed running and made significant changes in my diet. Now at age 72 I feel like I am the healthiest of my life. I don’t consume sugar and just a tiny amounts of seed oils and love the food I eat.
Thanks again for another enlightening and captivating piece. You are a treasure.
I did not know about the CCTA test so very good information.
GREAT article Dr. Cate! I have never been told to have any arterial scans (yet) but I think I am close due to my higher cholesterol which I don’t believe is a problem because I am otherwise very healthy. My Dad is 90 and has had high cholesterol his whole life and doesn’t take drugs for anything! Now that I know about this IF they do order a scan I will know what to ask for. Thank you so much for your research.
Under what circumstances would you recommend a statin?
Excellent article! As a widowmaker survivor I spent a lot of time trying to learn why I had a heart attack. I eventually learned about unstable (soft, inflammatory) plaques through reading and research. But unfortunately not much from the various cardiologists I had over time. One good source was the book ‘The Clot Thickens’, by Dr. Malcolm Kendrick.
Ten years post my heart attack, I do not take statins, but I exercise regularly, and eat healthy as directed by Dr. Cate Shanahan’s teachings. I am doing very welI and even compete in fitness competitions. I am very pleased to see this plaque information written up in an easy to read article.
I wrote a book on my experiences with my heart attack, and the aftermath, in a book ‘Widowmaker to Warrior’, which will be published very soon on Amazon.